Have you ever wondered who clinical embryologists are or what they do all day in the lab? The purpose of this article is to briefly review the tasks and skills of clinical embryologists in the laboratory. It will talk about the technique that they employ, which is called in vitro fertilization (IVF). It introduces procedures, methods, and equipments that they use in IVF to select and match the qualified sperm and oocytes. Then it explains the process that they follow for creating embryos, preparing a good environment for them to grow, transferring the best ones back into the female body, and deciding what to do with the rest. It indicates that controlling and maintaining quality in the lab is as important as other procedures for embryologists. Their decisions and techniques are very important in every step of the procedure and require precision.
A BRIEF REPORT OF THEIR JOB IN THE LABORATORY
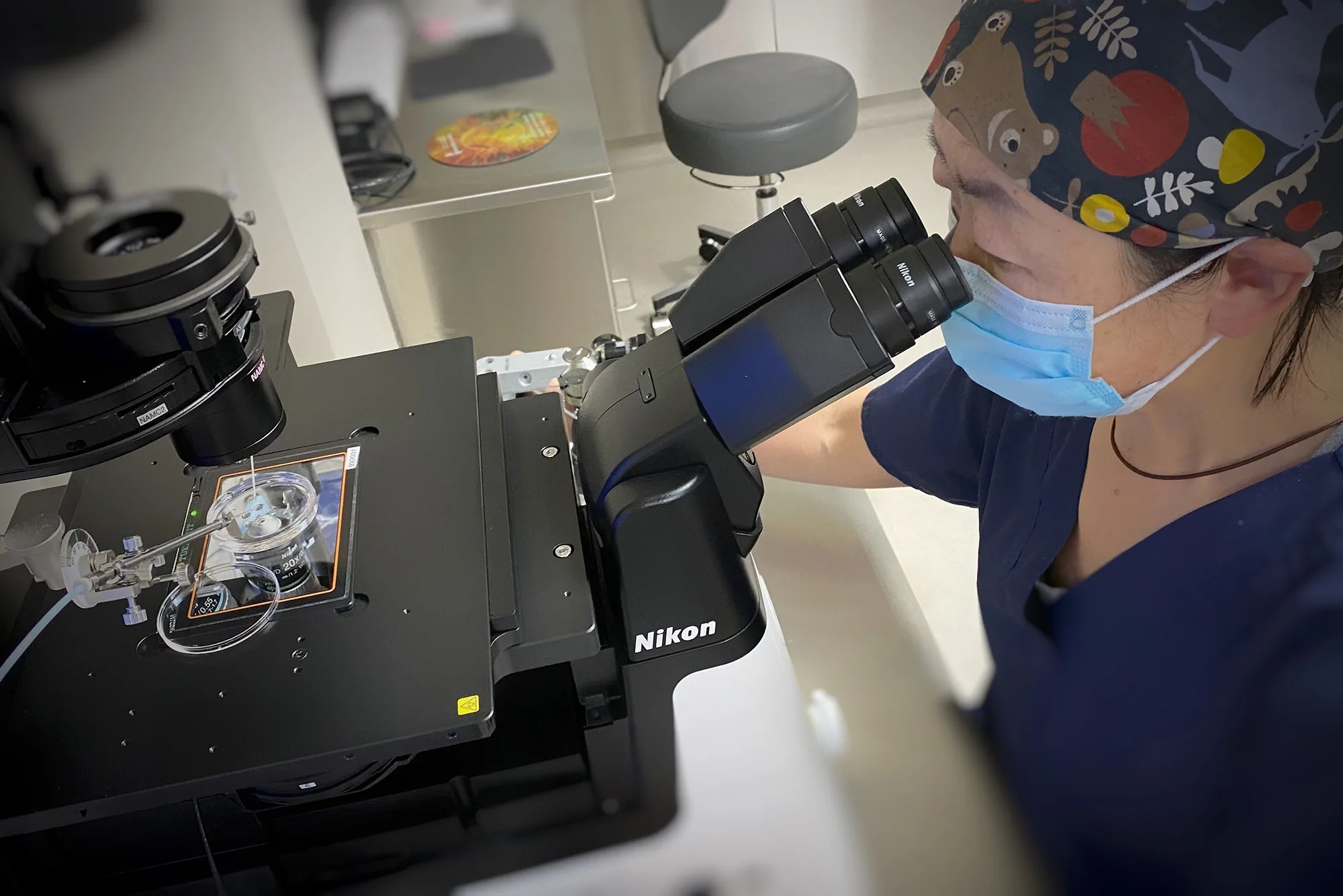
An IVF laboratory is the most important section in an IVF center because it is where most of these treatments happen. Therefore, all of the equipment, supplies, surroundings, and environment must be ready for the procedures. However, even when everything is ready, nothing could move forward without the hard work of highly qualified and experienced laboratory personnel, which in this case are called clinical embryologists.Clinical embryologists are scientists who spend most of their time and energy in the lab creating life. Their main goal is to help infertile patients to achieve their dream of having babies. They are busy the whole day in the lab, employing their micro-manipulation skills, checking carbon dioxide (CO2) incubators, transferring gametes and embryos from one culture medium to another with care, performing quality control in detail, and so on. Right after they receive the sperm and oocytes, embryologists try their best to make them ready for each other. They match the qualified sperm and oocytes and fuse them to create embryos. To do so, they follow certain procedures and rules meticulously.
OOCYTE COLLECTION AND GRADING
Before the physician starts the oocyte retrieval, embryologists make sure everything is ready for the gamete’s arrival. Everything should almost resemble the mother’s body. So they check the temperature of the room, incubators, and microscope stages. Also the room’s light must be dimmed at all time for eggs and embryos. All the culture media and dishes are prepared to welcome the oocytes. The physician aspirates the follicular fluid and oocytes and hands the aspirates and flushes, in the test tubes, to embryologists. Under the microscope, embryologists immediately examine the fluid and search for them. If they find them, they immediately wash them and transfer them to the fertilization medium that has been prepared for them, and then transfer them to the incubator for later checking and grading. Mature oocytes are placed in incubators for 2-8 hours until insemination. Immature oocytes need more time, around 24-35 hours, to get mature and ready for insemination (Jones, H., Jones, G., Hodgkin, & Rosenwaks, 1986).Grading oocytes depends on the way they will be inseminated. If conventional insemination is the method of use, they will be graded as they are, with both cumulus and corona radiata surrounding them. Usually the mature ones look like a beautiful sun with clear expanded rays around them. If the method of insemination is intracytoplasmic sperm injection (ICSI), the embryologist needs to examine the oocytes by themselves with no cumulus or corona surrounding them. To do so, they first mechanically clean the cells surrounding the oocyte with syringes and then for a few seconds strip them in an enzyme which is called hyaluronidase to complete cleaning. Hyaluronidase is an enzyme that is usually released by the sperm head during the process of fertilization, to dissolve the oocytes surrounding cells, and allow it to bind with oocyte.Now that the embryologist has a clear view of the oocytes under the microscope they can grade them. A spherical shape oocyte, with a polar body attached to it, is called mature and is ready for insemination in 2-8 hours. The oocyte that has spherical shape, but no polar body, would be called immature and should sit in the incubator for 24 hours to have chance to become mature. Also, if the oocyte is broken, or does not have spherical shape and polar body, it is considered abnormal and would be discarded.
SPERM PREPARATION AND GRADING
Sperm preparation is usually done by clinical scientists who work on male infertility and are called andrologists. However, if they are not available, embryologists can fulfill the role. Semen samples are processed with a technique to separate sperm from cells and debris. Usually sperm aspiration would take place by a physician if the male partner is not able to ejaculate or there is rare or no sperm in the ejaculate. Embryologists check the sperm quality and quantity and decide if they are suitable for fertilization or not. They check the sperm morphology to see if there is a normal or abnormal physical appearance, motility, concentration, and speed of their swimming. If the sperm quantity and quality are normal, they would be considered for conventional insemination. Otherwise, the sperm would be directly injected into oocytes because they are not able to penetrate the oocytes by themselves.
FERTILIZATION
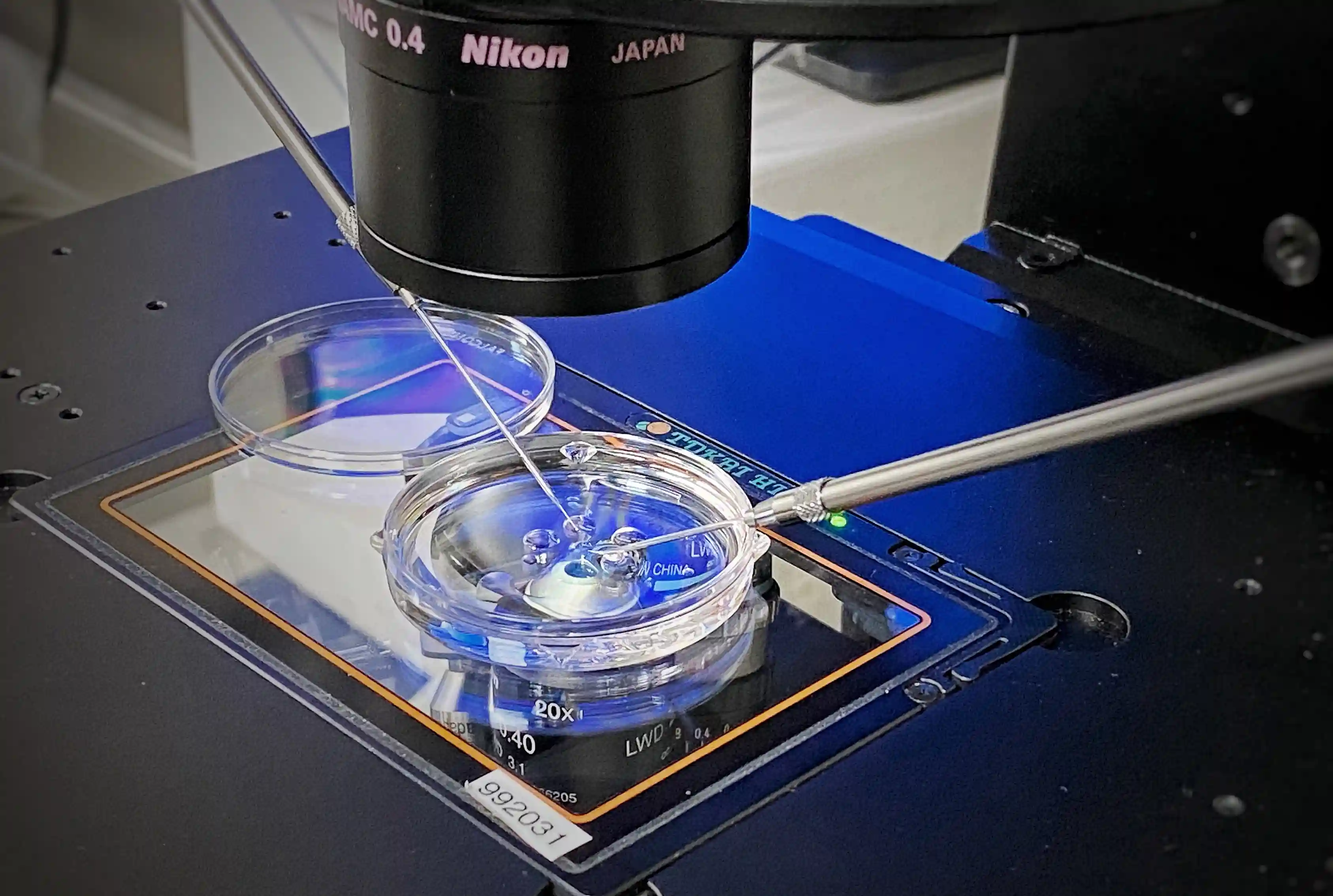
If the sperm is of good quality and quantity it will be used for conventional insemination; otherwise, ICSI would be performed. Conventional insemination means incubating mature oocytes with qualified sperm. Speroff and Fritz (2005) suggest that “In general, each oocyte is incubated with 50-100 thousand motile sperm” (p. 1234), to get the desired result. Therefore, embryologists incubate each oocyte with this amount of sperm, in a dish with fertilization medium, for about 12-18 hours. During this time fertilization may occur when a sperm penetrates the oocyte and they fuse together.ICSI would be done if the sperm quantity is low. ICSI procedure is very effective in IVF, Gardner, Weissman, Howles, and Shoham (2004) report that “The ability of ICSI to achieve higher fertilization and pregnancy rates regardless of sperm characteristic makes it the most powerful manipulation procedure yet with which to treat male factor infertility” (p. 171). Embryologists pick one sperm; immobilize it, drawing it into the pipette tail first so that the head can be inserted to the oocyte first. The oocyte should be stabilized on the other side so that the polar body is at 12 or 6 o’clock position. Then the embryologist injects the sperm head in 3 o’clock position inside the oocyte. After the injection, these oocytes also need to be placed in incubators for 12-18 hours.After 18 hours, embryologists check them to see if fertilization has happened. The result of fertilization is a cell which is called zygote. At this point the pronuclear status of the zygote needs to be examined. The zygote that was created by conventional insemination is covered by a layer of corona cells and they need to be removed to visualize the oocyte for grading. However, the zygote that is the result of ICSI is already clean. If the zygote is normal embryologists can see two pronuclei inside of it and two polar bodies on the surface. The two pronuclei are usually called 2PNs. Embryologists are always carefully examining the pronuclei, and if they see 3PNs, they know that zygote is not normal and discard it (Jones et al., 1986). The process of fertilization usually takes 24 hours and it ends with the first cleavage. The zygote is now called an embryo is called embryo.
CULTURING AND GRADING EMBRYOS
Embryologists make sure everything is ready for embryo culture. They make the environment ready so that the embryos feel that they are cleaving in their mother’s body. The media and its pH, embryo group size, oxygen and carbon dioxide are important in culturing embryos (Gander et al., 2004). Normally embryos cleave and reach 2 cell stage within 25-27 hours (day one) after insemination or ICSI. In 48 hours (day 2) they reach 4-6 cell stage, in 72 hours (day 3) 8 or more cell stage, on day 4 morula, and day 5 blastocyst.Grading system for day 1-3 could be different among different IVF centers but the main point is to consider the number of blastomeres or cells each day, the size of blastomeres, and degree of cytoplasmic fragmentation. Even sized blastomeres and minimal fragmentation means the quality of embryos are better. This grading is especially important if the transfer of embryos take place on day 3. Embryologists observe and examine each embryo very carefully every day so they can pick the best qualified embryos for transferring into the patient.If transferring doesn’t happen on day 3, then it goes on to day 5 when embryos turn to blastocysts. Generally, blastocysts get their grading according to their degree of expansion, status of hatching, inner cell mass (ICM) development, and their trophectoderm formation. A full blastocyst with tightly packed ICM and trophectoderm forming cohesive epithelium with many healthy cells usually would be considered a good candidate for transferring (Veeck and Zaninovic, 2003, p.104).
TRANSFERRING EMBRYOS
On transfer day, embryologist picks the best qualified embryo or embryos for the designated patient. When the patient is in the right position, the embryologist aspirates the embryo(s) into the catheter and hand it to the physician to transfer them into the uterus. When the transfer procedure is completed, the physician gives the catheter back to the embryologist to flush it and examine the material. This way they make sure that the embryo(s) has been transferred successfully or not. If, by any chance, any embryo returns in the catheter, they will repeat the procedure over again.
CRYOPRESERVATION AND THAWING
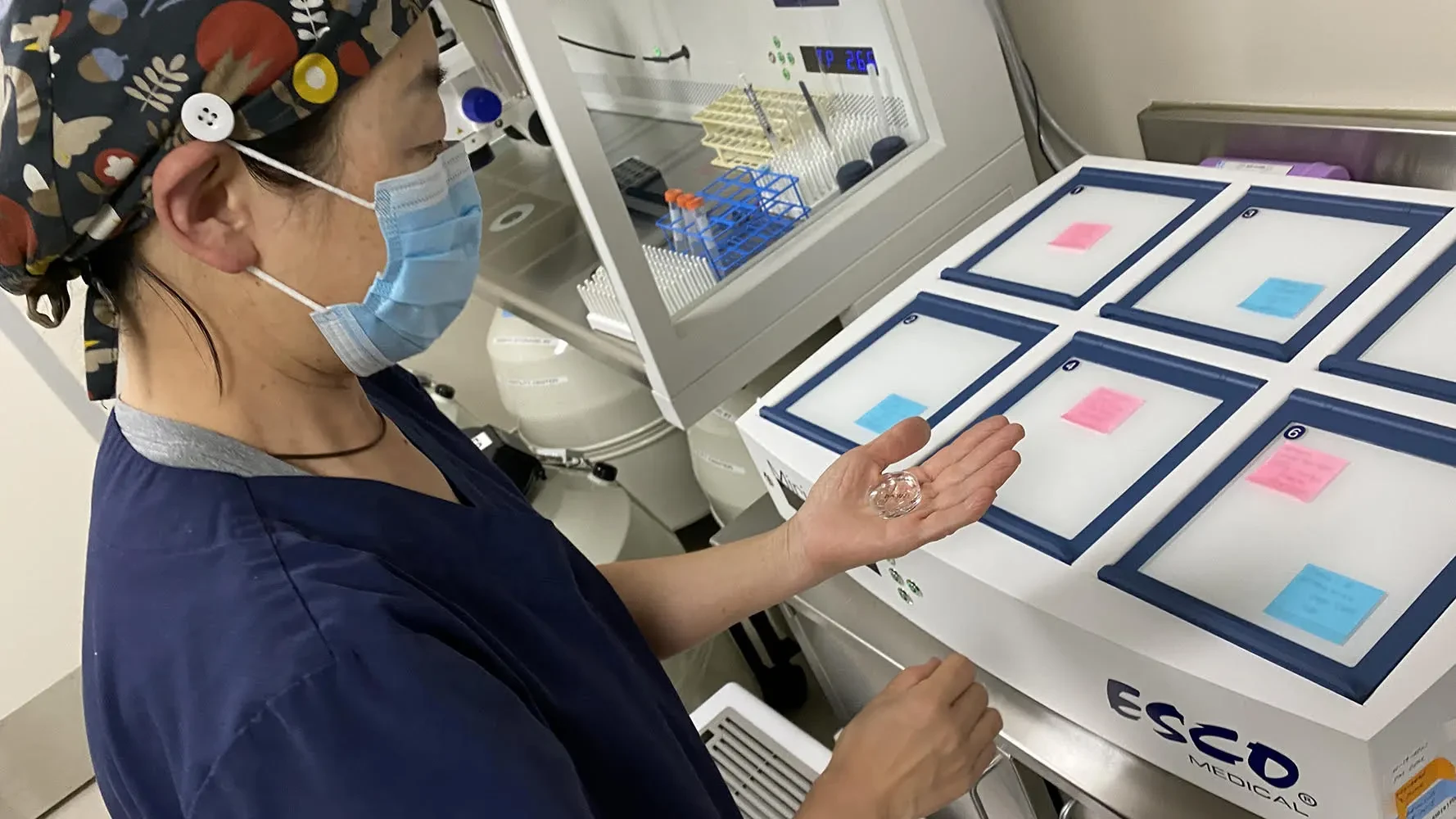
Cryopreservation or freezing and thawing or unfreezing of gametes (eggs & sperm), zygote, and embryos allows more chances of pregnancy from one egg harvest. Most of the time patients end up with excess embryos and embryologists suggest cryopreservation. Freezing embryos give the patients opportunity to decide if they want to use them in future. Some centers freeze the extras when they are zygotes with 2PN and some freeze at blastocyst stage. However, Gardner et al., (2004) state “Embryos freeze well and implant at acceptable rates after thaw and transfer. Almost any cleavage-stage specimen can be frozen successfully, from 2-cell to blastocyst. Freezing the embryo is fairly convenient because there is no urgent timing considerations” (p.270). Freezing sperm is usually the andrologists’ job and they freeze the semen which is the male reproductive fluid that contain sperm. Oocyte freezing could be a big help to many who have problems with embryo freezing. However, freezing oocytes has not been easy due to the unique biological feature of oocytes. Recently, a new technique, which is called vitrification, has shown promise for oocyte freezing. In some IVF centers embryologists have started using this technique with fair results more studies are needed to optimize the technique (Gardner et al., 2004).
PREIMPLANTATION GENETIC TESTING
Preimplantation Genetic Testing (PGT) refers to procedures that could evaluate oocytes or embryos before implantation. It helps many couples who are at risk of having children with inherited genetic abnormalities. It also reveals the sex of the embryos. If couples are interested, embryologists can remove one or more cells from embryos for later evaluation. The procedure is very sensitive and embryologists must be highly skilled in micromanipulation to be able to remove the cell without causing damage to the embryo. The cell would be chromosomal analyzed and the results reported to the embryologists. If embryos are abnormal the embryologists notify the couples and they can choose whether or not to discard them.
QUALITY CONTROL
One of the most important tasks of embryologists is controlling and maintaining the quality of the embryology laboratory. According to Cutting, Pritchard, Clarke, and Martin to maintain high standard of practice in IVF laboratories, embryologists need to establish a quality control system (2004). For example all the equipment should be checked and receive maintenance regularly. Hoods should get cleaned routinely and incubators’ temperature, carbon dioxide, water pan level, and their alarm should be set and checked. According to Mayer et al. (2003) “An example of common QC is documentation of refrigerator temperature on a daily chart. These measurements are compared to a range of acceptable limits that had been previously defined” (Introduction section, para. 1). All the materials must be free of toxicity therefore embryologists test all of them before using them. Most laboratories use “Mouse Assay” to check the quality of materials. Most of the materials that are in contact with human gametes and embryos like solutions, culture dishes, catheters, and such get tested. Two-cell mouse embryos are cultured in these items, in the same manner as human embryos, and the results are monitored. Embryologists watch to make sure mouse embryos growth from the two cell stage to the hatched blastocyst stage. If a certain number of mouse embryos do not reach the blastocyst stage, the item fails. In this case those materials that fail the test will be sent back to their company.
CONCLUSION
Many infertile patients around the world find themselves in the IVF centers with the hope that their dreams of having babies come true. The fundamental part of any IVF center is embryology department where clinical embryologists work. Clinical embryologists are diligent scientists who use their skills to fulfill their sensitive tasks. Their tasks consists of egg collection, sperm preparation, gametes and embryos grading, fertilization, culturing embryos, transferring embryos, freezing & thawing of gametes and embryos, PGD, and quality control. They need to follow the procedures step by step precisely. Every step is a challenge and needs highly qualified embryologists to achieve satisfactory results.
REFERENCES
1.Cutting, R. C., Pritchard, J., Clarke, H. S., & Martin, K. L. (2004). Establishing quality control in the new IVF laboratory. Human Fertility, 7(2): 119-125.2.Gardner, D. K., Weissman, A., Howles, C. M., & Shoham, Z. (Eds.). (2004). Textbook of assisted reproductive techniques: Laboratory and clinical perspectives (2th ed.). Landon, New York: Taylor & Francis.3.Jones, H. W., Jr., Jones, G. S., Hodgkin, G. D., Rosenwaks, Z. (Eds.). (1986). In vitro fertilization. Norfolk: Williams & Wilkins.4.Mayer, J.F., Jones, E.L., Lacy, D.D., Nehchiri, F., Muasher, S. J., Gibbons, W. E., & Oehniger, S. C. (2003). Total quality improvement in the IVF laboratory: Choosing indicators of quality. Reproductive BioMedicine Online, 7 (6), 695-699. Retrieved from http://www.rbmonline.com/article5.Speroff, L., Fritz, M. A. (2005). Clinical gynecologic endocrinology and infertility (7th ed.). Philadelphia: Lippincott Williams & Wilkins.6.Veeck, L. L., Zaninovic, N. (2003). An atlas of human blastocysts. New York, London: The Parthenon Publishing Group.Dr. Azita Hengameh NazariBack to blog >